Good night. I’m Karen Kaplan and it’s Tuesday, January 31. Here’s the latest news on what’s happening with the coronavirus in California and beyond.
For months now, almost everything similar to the pandemic seemed to be improving. At times, this progress has happened intermittently, but the momentum shifts in only one direction: toward the day when we can safely treat COVID-19 like any other. infectious disease.
Then I received a sobering reminder about how difficult it is to keep up with the ever-changing coronavirus.
The message was conveyed through the U. S. Food and Drug Administration. U. S. On Thursday, the company revoked its emergency use authorization for Evusheld, a reference drug relied on by millions of Americans with weakened immune systems to prevent them from becoming seriously ill if they contracted COVID-19.
Evusheld obtained FDA approval in December 2021. This is a mixture of two monoclonal antibodies, tixagevimab and cilgavimab, which can be injected directly into patients struggling to produce antibodies on their own, even after multiple injections of the COVID-19 vaccine. With the medication that gives them the coverage they needed, they can finally get out of isolation from their homes and rejoin the world without risking their lives.
Now that coverage is gone.
“It’s a sad time,” Dr. Anna Healy told my colleague Melissa Healy. Camille Kotton, a physician at Massachusetts General Hospital. more and we may not be able to update them with anything. “
Evusheld’s disappearance is due to the Omicron variant, the maximum foxy iteration of the coronavirus to date. Nine subvariants of Omicron, totaling XBB. 1. 5, BQ. 1 and BQ. 1. 1, involve mutations that allow them to escape drug coverage. It is intended to provide.
Unfortunately, those nine subvariants together account for more than 90% of the coronavirus samples recently circulating in the country, according to estimates by the Centers for Disease Control and Prevention. Withdraw your emergency use authorization.
It’s possible that Evusheld will be restored if the proportion of resistant variants falls below 90 percent in the future, the FDA said. But for the moment, that doesn’t seem likely. This means that a drug whose progression and production will cost taxpayers at least $1. 58 billion will be obsolete in just over a year.
It’s not the only anti-COVID drug to die through genetic modifications of the coronavirus. The Delta variant was the first in a monoclonal antibody therapy, and Omicron eliminated most of the others. Of seven antibody remedies in the past eliminated through the FDA, only one, tocilizumab, is still available, but only for critically ill patients who are being treated in a hospital.
The loss of those antibody treatments is serious considering the fact that many other people with weakened immune systems cannot take Paxlovid as it would stop other medicines they are taking. This leaves them with two lower-than-normal alternatives: molnupiravir, a less effective antiviral than Paxlovid, and remdesivir, which requires 3 days of infusions, in a hospital.
All of this represents a huge step backwards for the estimated 7. 2 million immunocompromised American adults. These are other people undergoing cancer treatment; other people who take medicines to prevent their immune formula from rejecting transplanted organs; other people with autoimmune diseases such as rheumatoid arthritis; and others who have lost critical T cells due to complex or untreated HIV, among others.
Evus used to be given to patients once every six months. But some other people gained only one dose before the drug lost its effectiveness. Some had never taken it.
“We mourn the official death of what had been a tool,” Kotton said.
We’re not going to get out of this pandemic by letting setbacks derail our progress. AstraZeneca, the company that makes Evusheld, said Friday it is in a position to develop a new antibody drug for others with weakened immune systems. The pharmaceutical giant expects the new drug to be in condition until the end of the year.
Case and in California at 5:15 p. m. Tuesday:
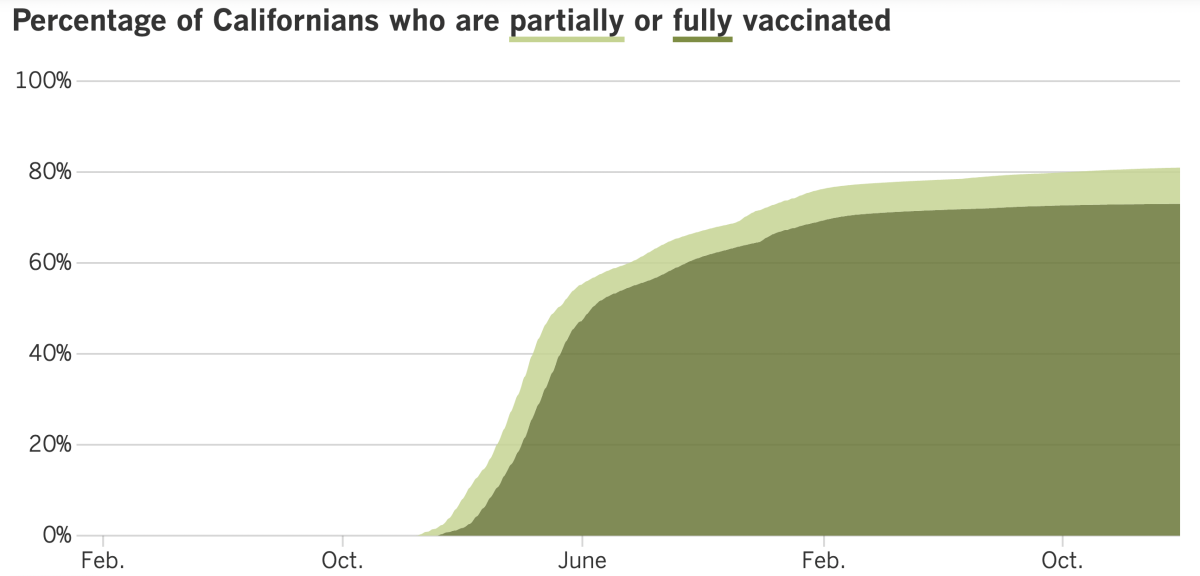
Track California’s coronavirus and vaccination efforts, adding the latest numbers and their breakdown, with our charts.
The most recent CDC figures show that only 16. 5% of Americans over the age of five have gained the newest COVID-19 boosters, launched in September and specially formulated to recognize the Omicron variant. to mention over $1 billion in fitness prices in the U. S. alone. In the U. S. ), we obviously want to make it as simple as possible.
mRNA vaccines made through Pfizer-BioNTech and Moderna are about to become more expensive. Will it make injections more available or will it have the opposite effect?
If you’ve ever taken a fundamental economics course, or if you have a modicum of common sense, you know the answer is obvious: increasing the value of COVID-19 vaccines will mean fewer people will be able to do it.
The value building we are talking about is substantial. The federal government has purchased 1. 2 billion doses of the Pfizer and Moderna vaccines, paying an average of $20. 69 each, according to Kaiser Family Foundation estimates.
But Congress has stopped allocating cash for products essential to the pandemic, such as vaccines. Soon, corporations will sell their vaccines to health care providers and negotiate costs with insurance corporations. Moderna and Pfizer have announced they plan to charge between $110 and $130 depending on the dose. That’s an increase from 432% to 528%.
Most Americans would not pay the full value of the label. In fact, if they have health insurance, they wouldn’t give cash when they rolled up their sleeves. (That’s thanks to the Affordable Care Act, which encourages preventive care. )
But they would pay the higher value indirectly, through higher insurance premiums. And other uninsured or underinsured people may enjoy a surprise.
As my colleague Michael Hiltzik reports, corporations have defended their increases in value through the massive savings imaginable from their vaccines.
The company’s Pfizer vaccine, Comirnaty and the Paxlovid antiviral tablet have “saved thousands of lives [and] tens of billions of dollars in health care costs,” a Pfizer spokesperson told Hiltzik. The company “has set the value of the vaccine at that value is consistent with the cost provided,” the spokesperson added.
A spokesperson for Moderna echoed this theme: “Moderna is committed to providing awards that reflect the COVID-19 vaccines they provide to patients, healthcare systems, and society,” he said.
Hiltzik wonders why corporations deserve to make a decision about how much of those savings deserve to be directed to them, especially since mRNA vaccines were made imaginable through taxpayer-funded fundamental research. Moderna also won a direct grant from the federal government’s Department of Biomedical Advanced Research and Development. The authority values nearly a billion dollars.
“It is exaggerating the ethical depravity of this argument,” Hiltzik wrote.
In fact, he wonders why companies want to increase the value of their vaccines.
Oxfam International, an anti-poverty nonprofit, used an inconsistent report from Imconsistent withial College London to estimate that the Pfizer vaccine can be produced for as little as $1. 18 according to dosage, while the Moderna vaccine can be manufactured for only $2. 85 consistent with dose. Even if corporations kept their value solid at $20. 69, their profit margins would still be enviable.
Since federally funded studies have contributed to the realization of mRNA vaccines, the government has the strength to influence its Bayh-Dole Act costs. Among its provisions are “entry fees,” which allow the government to take action if a company that studies taxpayers does not implement its product on “reasonable terms. “
The federal government has threatened to use its access fees in the past, but has never acted on it. But there’s a first for everything, and given the critical importance of COVID-19 vaccines, it will be that.
“Few drugs on the market today can adapt to their ability to promote public health and few can be as delicate to the point of the value increases projected by Moderna and Pfizer,” Hiltzik writes. “This is an issue where the government cannot and will not remain silent. “
Discover advances in vaccination in California with our tracker.
Friday marked the third anniversary of Los Angeles County’s first coronavirus infection. Barbara Ferrer, the county’s director of public health, marked the moment by sharing some undeniable smart news.
The nation’s most populous county now averages less than 1,000 official cases per day. (On Tuesday, that number was 931. ) In addition, viral levels detected through water monitoring have dropped dramatically in recent weeks.
“These figures verify that the decrease in transmission is real and significant,” Ferrer said.
Los Angeles continues to have a low network point of COVID-19, with the number of cases declining by nearly 22% week over week, according to the CDC. (In fact, almost the entire state of California is lately in the “weak” category. The exceptions are San Diego and Imperial counties, which are classified as “average. “)
The number of COVID-19 deaths, about 136 countywide over the past week, remains too high. In early November, before the holiday season began, the weekly death toll stood at 43. Start the wave of Omicron moment, there is a week with only 24 deaths.
Ferrer said he hoped “the decline in transmission will soon be followed by a reduction in deaths. “Good,” he added.
The recent progress is due to a combination of factors, Ferrer said, adding COVID-19 vaccines, immunity beyond infections, drugs that work, preventative measures like wearing a mask in crowded public spaces and a willingness to stay home when coronavirus control is shown. infection.
Local situations have advanced so far that the county has replaced its general council so that grocery stores, libraries and other public places are covered up. Instead, for most people, the decision to wear a mask is now a matter of private preference.
Ferrer said other people who are at risk for a severe case of COVID-19 continue to wear masks indoors, especially in crowded or poorly ventilated places. The same recommendation applies to other people living with a vulnerable person. Masks remain mandatory for everyone when taking public transport or spending time in in-house medical services or nursing homes.
Ferrer, the only official who felt positive those days. President Biden told Congress on Monday that the nation’s public fitness emergency would end on May 11.
The physical emergency was first declared by then-President Trump on January 31, 2020, and has been extinguished each and every month since. Trump also decided that the pandemic presented a national emergency on March 13, 2020. ; which will also end on May 11.
Once emergencies are officially over, at least on paper, the government will manage coronavirus risk through its general channels. Vaccines, tests, and remedies will no longer be loose (although investment for the pandemic is low and Congress doesn’t need to take more ownership of them, those things will have to keep them from being released anyway).
These aren’t the only adjustments we’re hoping for. All emergency use authorizations granted by the FDA will no longer be valid, so the only vaccines and remedies that will remain available are the few that have obtained full FDA approval. receive more investments to care for COVID-19 patients. The health insurance budget would likely avoid paying for telemedicine visits. And millions of Americans may also lose their fitness insurance altogether as Medicaid’s patient policy falls by the wayside.
The World Health Organization also considered the duration of the public physical emergency. After meeting with key advisers on Friday, company officials decided it was still too early to set an end date.
“There is no doubt that we are in a much greater situation now” than we were a year ago, WHO Director-General Tedros Adhanom Ghebreyesus said on Monday. But more than 170,000 people have died from COVID-19 in the past eight weeks. , some countries still suffer from vaccines and medicines, and misinformation is undermining efforts to control the pandemic virus.
The end is still in sight, but it may be soon. The WHO’s advisory committee said the pandemic “may be reaching a tipping point,” and Tedros agreed.
“We are hopeful that, in the coming year, the world will move into a new phase where we reduce hospitalizations and deaths to the lowest level imaginable,” he said.
Today’s comes from readers who need to know: Is the threat of dying from COVID-19 even greater for other unvaccinated people than for other vaccinated people?
This consultation comes from a reader whose unvaccinated enjoyees insist that COVID-19 is so mild that vaccination is no longer mandatory. These enjoyed might be surprised to learn that even 3 years after the outbreak, they are getting their initial doses now. It will still be assistance — a lot.
At the end of November, there were 1. 79 deaths from COVID-19 corresponding to 100,000 unvaccinated Americans, according to the CDC. That might sound small, but it’s more than five times higher than the COVID-19 death rate for Americans who were vaccinated. fully vaccinated but did not get the new booster targeting Omicron (0. 35 consistent with 100,000). It’s also more than 11 times higher than the COVID-19 death rate for Americans who won the new bivalent retirement (0. 16 consistent with 100,000).
If you’re looking for information near you, those numbers from Los Angeles County: Between Dec. 5 and Jan. 3, the COVID-19 death rate was 16. 6 deaths, which equates to 100,000 unvaccinated residents, or just under five deaths, which equates to 100,000 people who were vaccinated but did not receive the updated booster and 2. 3 deaths consistent with 100,000 population who were vaccinated and recently reinforced.
One thing family members are right about is that vaccine mortality is higher.
A study published last year by the CDC estimated that the risk of death from COVID-19 was nearly 22 times higher for the unvaccinated than for those vaccinated in April and May 2021, before the Delta variant arrived. In the Delta era, COVID-19 mortality rate for the unvaccinated 16 times higher than for the vaccinated. And at the height of the Omicron surge last winter, COVID-19 killed other unvaccinated people at a rate 10 times higher than vaccinated people, according to other CDC data.
We need to hear from you. Please email us your coronavirus inquiries and we will do our best to answer them. Wondering if your inquiry has already been answered? Check out our archives here.
The woman pictured above is Amy McCoy, owner of Forever Young daycare in Mountlake Terrace, Washington. Declining U. S. Birth Ratedespite everything reversed in the current year of the pandemic, according to a report released today through the CDC’s National Center for Health Statistics.
A final count of birth certificates concluded that the country’s overall fertility rate in 2021 was 56. 3 births consistent with 1000 women of reproductive age (i. e. , between 15 and 44 years old). This is an accumulation of 1% since 2020, when there were 55. 7 consistent births with 1,000 women of reproductive age.
More importantly, this is the first construction of its kind since 2014.
The total number of young children born in the U. S. The U. S. economy in 2021 (3,664,292) is also 1% higher than in 2020 (3,613,647). Before that, the number of births had plummeted 4% in the first year of the pandemic after falling from 1% between 2014 and 2019.
The CDC report does not mention COVID-19, but each and every child born in 2021 was conceived after lockdowns began in March 2020. Perhaps when the information arrives for 2022, statisticians will have a better idea of the role of the pandemic. in the country’s investment. Bust of baby almost ten years old.
Followi
Karen Kaplan is scientific and medical editor at the Los Angeles Times. Before joining the clinical group, he worked in the Business section. He graduated from MIT and Columbia University.
Subscribe to access Site Map
Followi
MORE FROM THE TIMES